Rail DiMeC研究会の英文名は、Research group on utilization of railways for disaster medical careです。
私は、医療レギュラトリーサイエンス研究所の初代所長で、定年退職後、この研究所の顧問となりました。現役時代、国立循環器病センター研究所の設立スタッフ、シドニー・セントビンセント病院でのオーストラリア人工心臓開発プロジェクトリーダーを経て、本学の医工連携の推進のコアメンバーとして、50年にわたり人工臓器の研究・評価開発に携わりました。また、定年前の15年間、稲門鉄研会長を務めており、鉄道への思いは強く、70歳で退職後、医療と鉄道を結び付けようと考え、この研究会を立ち上げました。
2. Rail DiMeC研究会の発足
たまたま、私が所属する一社)スターリサーチャーの兵庫県での講演会で、災害医療支援に鉄道が活用できないか、という話題を提供しました。その時、複数の災害医療専門医から「ぜひ一緒に活動したい」という希望がだされました。そして2023年5月に開催された日本生体医工学会の総会で、私の友人で一社)スターリサーチャー代表の生田幸士東京大学名誉教授から「防災医工学」という新たな専門別研究会を提案し、承認していただきました。そこでは、災害医療関係者、大学関係者、医療機器・鉄道車両や自動車メーカー、倉庫業者、物流事業者、鉄道事業者などの異分野の方々にもご協力いただき、まさに連携チームの活動が活発になってまいりました。この活動を今まで1年半にわたりサポートいただいてきた本研究所のメンバーは、岩﨑清隆所長、宮田俊男教授、松浦由佳博士、笠貫宏顧問、そして、この機会に招聘研究員になっていただいた小峰輝男氏です。彼は、早稲田大学機械工学科の卒業生で、新幹線のぞみ300系の開発に中心的にかかわった鉄道技術者です。今になって、人の繋がりの神秘さと重要さを痛感しています。
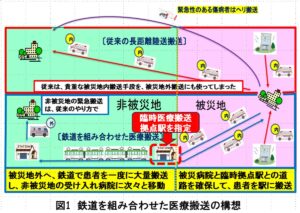
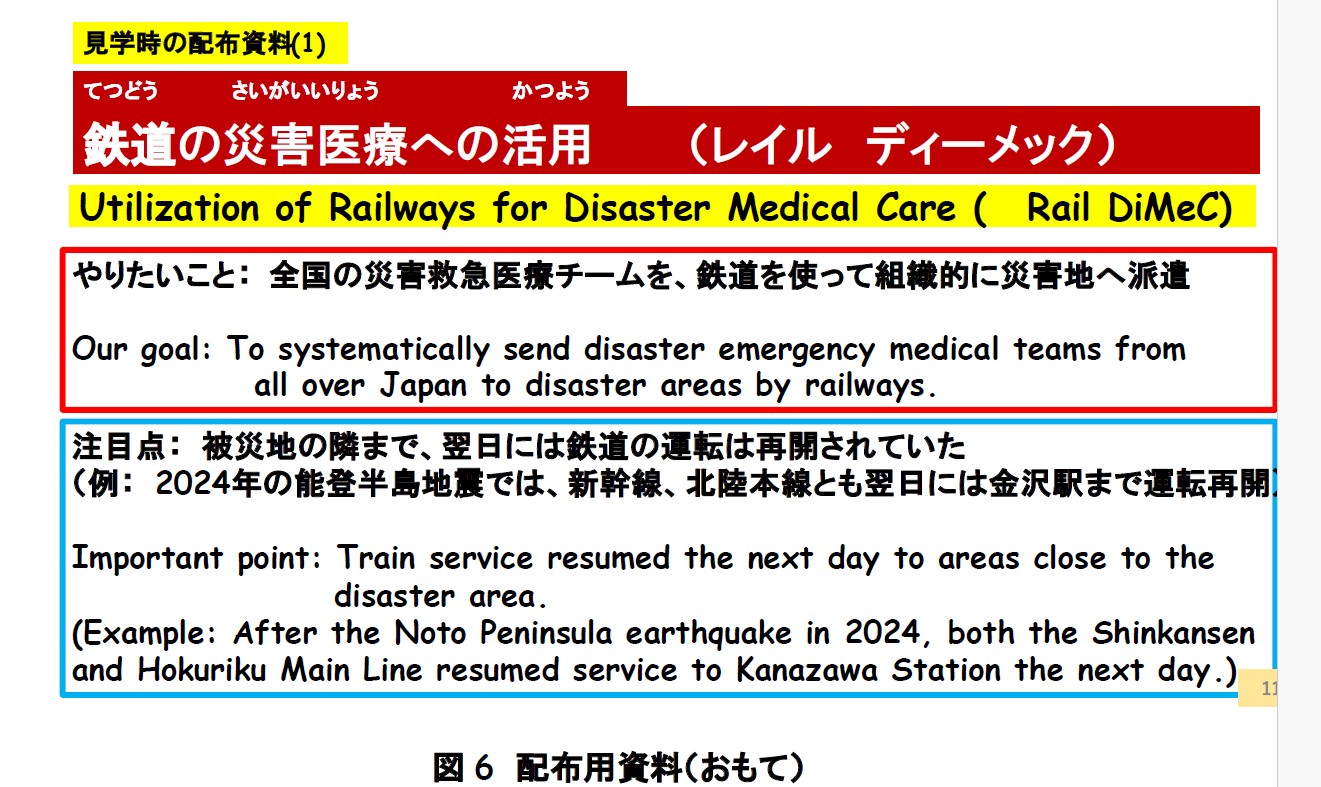
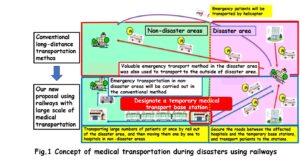
3. 大規模災害発生時に鉄道の価値はどこにあるのか 今まで、大地震など大規模災害発生時の被災者の搬送は、空路はドクターヘリや自衛隊の輸送機、陸路は救急車や自衛隊車両によって行われ、鉄道の活用はほとんど考えられていませんでした。被災地からの報道は、倒壊した建物や脱線した電車などのセンセーショナルな映像が紹介されますが、Rail DiMaC研究会は被災していないぎりぎりのところまで、翌日には鉄道が再開されている事実に着目しました。そこで、図1のような鉄道を活用した医療搬送の基本構想を考えました。図の右が被災地、左が非被災地で、その境界に、赤で示したような、臨時の医療搬送拠点駅を指定します。莫大なニーズの災害派遣医療チーム(Disaster Medical Assistance Team,略称DMAT)を迅速に組織的に被災地に送ることや、被災地の傷病者を安全に非被災地へ運び出すことは、この臨時拠点を作ることで、より多くの災害弱者を救済し、未治療被災者を減らすことが可能になると考えました。
by Rail DiMeC Group (Project leader: Mitsuo UMEZU, PhD. Professor Emeritus of Waseda University, umezu@waseda.jp)
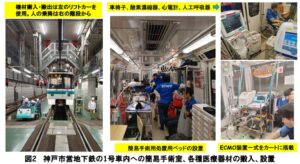
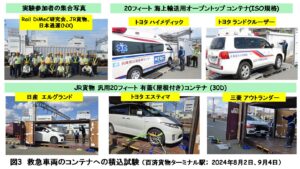
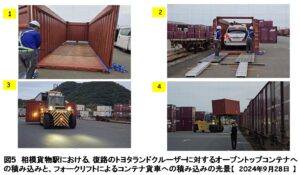
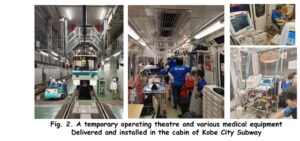
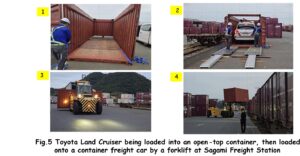
I served as the president of Waseda University’s railway fan club for 15 years until my retirement. After retirement, I thought about combining medical care and railways and founded the “Rail DiMeC Research Group” to investigate the use of railways in disaster medical care. Hospital trains first appeared during World War I to transport wounded soldiers from the battlefield. Currently, they are used to transport wounded invdivisuals in Ukraine during wartime, and have also been utilized for transporting COVID-19 patients via the French bullet train TGV. In Europe and China, fire engines and ambulances are loaded onto trains. In contrast, in Japan, transportation of victims of major earthquakes and large-scale floods is carried out by air using doctor helicopters and Self-Defense Force transport aircraft, and by land using ambulances and Self-Defense Force vehicles, and the use of railways has not been considered. We focused on the fact that railways were able to resume operation the next day up to the boundary of the disaster-affected areas. Therefore, we decided to designate temporary medical transport base stations on the border between the affected and non-affected areas, and to use them as starting points to quickly and systematically send disaster medical teams to the affected areas, which are in huge need. (Fig.1) On the other hand, we thought that by safely transporting a large number of injured and sick people from disaster-stricken areas to non-disaster areas, we could rescue many of those who are vulnerable to disasters and alleviate the strain on medical care in the disaster-stricken areas. Over the past year and a half, we have conducted experiments using actual trains to evaluate their potential in medical disaster care. The photos below illustrate these experiments in detail. (Fig.2-5)